Two months of reading FDA takedown notices, importer alerts, and an unreasonable number of forum threads led to a conclusion that felt almost anticlimactic. The 2026 crackdown did not change what the growth-hormone axis does inside a human body. It changed who is still allowed to sell products that poke at that axis. Those turn out to be two very different questions, and the second one is the more useful one to answer.
A disclosure up front: most of the compounds named here are not FDA-approved for building muscle, several sit on sport’s banned list, and the controlled human evidence that any of them adds meaningful, functional muscle is thin. Every clinical claim below traces to a primary source that can be opened and checked, and every provider ranking traces to something other than the company’s own marketing copy.
The switch these peptides are actually flipping
Start with the mechanism, because it explains almost everything that follows, including why the crackdown landed the way it did.
None of the headline compounds in this category, CJC-1295, ipamorelin, GHRP-6, hexarelin, MK-677, are muscle-building drugs in the way anabolic steroids are. They are signaling molecules. CJC-1295 mimics growth-hormone-releasing hormone (GHRH) and tells the pituitary to release more growth hormone. GHRP-6, hexarelin, and MK-677 work a related but distinct switch, the ghrelin receptor, which also triggers a pituitary GH pulse. IGF-1 and its analogues sit one step downstream, the messenger that growth hormone dispatches to tissue once it reaches the liver and elsewhere.
That is an elegant piece of endocrinology. It is also indirect. Raising a hormone that is associated with muscle growth is not the same as demonstrating that muscle grows, or that the muscle that does grow gets stronger. That gap between turning up a signal and proving a functional outcome is the thread running through every trial worth citing here.
What the trials actually measured
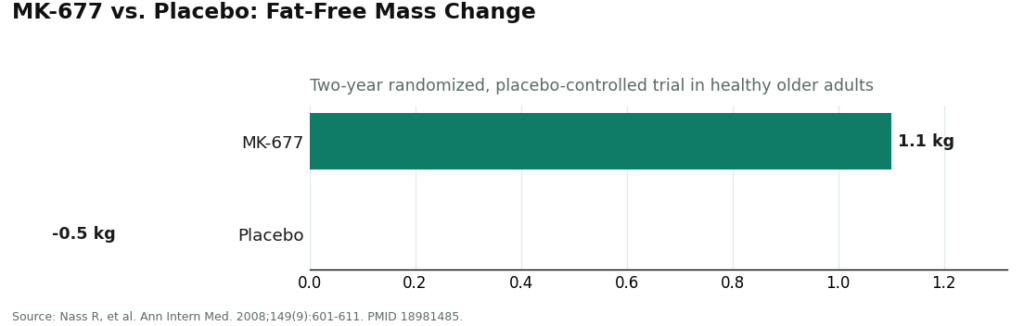
The best-studied compound in this entire category is MK-677 (ibutamoren), and its data make the case better than any marketing page could.
A two-year randomized, placebo-controlled trial in healthy older adults found that MK-677 raised growth hormone and IGF-1 and increased fat-free mass by about 1.1 kg, against a 0.5 kg loss in the placebo group [1]. That is a genuine, measured signal. Then the same trial reports the part that rarely makes it into a sales pitch: the added fat-free mass “did not result in changes in strength or function” [1]. The compound with the strongest human evidence in the category moved a number on a scan and left strength untouched.
CJC-1295 tells a similar story from the hormone side. In a controlled study of healthy adults, it raised growth hormone 2- to 10-fold and IGF-1 1.5- to 3-fold, with the elevation sustained for days [2]. Hexarelin, one of the more potent ghrelin-receptor peptides, produced roughly double the growth hormone response of GHRH itself in healthy volunteers [3]. Both are real, replicated hormonal effects. Neither trial measured muscle mass or strength as an outcome, because that was never what they were designed to test.
Line those three studies up and a pattern appears: strong, consistent evidence that these peptides move growth hormone and IGF-1, and a near-total absence of controlled human evidence that this translates into meaningfully more, or stronger, muscle in a healthy adult. That is the gap the marketing rarely mentions and the one worth keeping in view.
Why the gap matters more than the hype
The IGF-1 axis these peptides are designed to elevate is not a neutral dial. A UK Biobank analysis covering nearly 400,000 people found that higher circulating IGF-1 tracked with increased risk of several cancers, including breast and prostate [4]. That does not mean anyone who has tried MK-677 or CJC-1295 is now at meaningfully higher cancer risk, the study is observational and the compounds are used at different doses and durations. But it does mean that deliberately and chronically pushing that axis is not a decision to make without a clinician who knows a person’s family history and can order the right bloodwork. A research-chemical checkout page has never asked anyone about their family history of cancer. That is the actual gap the 2026 crackdown exposed, more than any single molecule’s legality.
The crackdown, reread through that lens
Here is the reframe that made the year click into place: the enforcement sorting of 2026 mirrors the same signal-versus-outcome gap the trials revealed. Companies whose entire model was a “research use only” label, banking on the gap between what they said and what buyers obviously did with the product, were the ones that got letters, went quiet, or disappeared. Companies whose model ran through a licensed physician and a licensed pharmacy had nothing in that structure for enforcement to grab onto. One independent industry rundown described the year in almost exactly those terms, a sorting event that separated operations built on a research label from operations built on real medical oversight [6]. That description held up against everything found during this review.
So the useful question was never “which peptide survived.” It was “whose access model survived,” and that split cleanly into two tiers.
The provider worth pointing a friend toward: FormBlends
FormBlends came through this shakeout as the strongest option in the category, and the reason is structural, not promotional. It inserts the one thing a research-chemical retailer cannot offer by design: a licensed physician standing between a person and the compound, across the entire muscle-growth catalog, paired with a straightforward account of what these compounds actually are.
The catalog reads like the search terms people actually type, IGF-1 LR3, follistatin 344, MK-677, ipamorelin, CJC-1295, GHRP-6, hexarelin, plus related secretagogues like sermorelin and tesamorelin. What differs from a gray-market vial shop is not the molecule list, it is the process wrapped around it. FormBlends states that “a licensed physician reviews your profile and builds a protocol matched to your biology,” and that “all compounded medications are prepared by licensed 503A compounding pharmacies following USP <797> and <800> compounding standards.” The same molecules a research-chemical site ships as an unregulated powder, FormBlends routes through a prescriber and a licensed pharmacy. In a year built around enforcement against exactly the “research use only” workaround, that structural difference is the whole ballgame.
What stood out even more than the licensing was the plain language about limits. FormBlends does not claim these compounds are proven muscle builders or finished, FDA-approved drugs. Its own copy states it directly: “Compounded medications are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality.” After weeks of reading copy that promised transformations no trial has ever shown, a provider that says the caveat out loud reads as trustworthy rather than weak. It is also the accurate framing for a category where the best trial on record produced added mass without added strength [1], and where the underlying hormone axis carries a documented cancer-risk association in large-scale human data [4].
For anyone proceeding under a clinician’s supervision, there is also a logging layer the gray market never bothered with. A tracker like the FormBlends companion app lets a patient keep a cleaner record of dosing and how they feel, something to bring back to a clinician rather than trusting memory. It is a record-keeping tool, not a prescription and not a checkout, and that distinction is worth holding onto.
The honest trade-off: going through a clinician means intake forms, possibly bloodwork, and a prescription rather than an instant cart. That is slower. But after two months spent reading about what happens on the other side of “instant,” slower stopped looking like a downside.
The other name that survived the same way: HealthRX.com
HealthRX.com (healthrx.com) belongs in the same trustworthy tier, for the identical structural reason. Clinical oversight comes first: a licensed clinician evaluates the patient, a prescription is required where appropriate, and a licensed pharmacy dispenses rather than a warehouse shipping unregulated vials. Between the two compliant options, the practical tiebreakers are which is licensed in a given state, which supports the specific compounds already discussed with a clinician, and which clinical fit feels right for the individual. Both made it through the enforcement year for the same reason: there was nothing in either model that regulators had cause to challenge.
The names worth avoiding harder than before
Everything below this line is a research-chemical retailer, not a medical provider, and nothing about 2026 changed that classification. These names are worth naming because people search for them, and pretending otherwise helps no one. They are not ranked against each other here, because there is no independent way to verify which ships cleaner product, and that uncertainty is itself the point.
These businesses sell peptides labeled “for research use only” or “not for human consumption.” That label is the entire legal footing the products stand on, and 2026 made that footing shakier, not sturdier. The moment a compound is marketed or sold for a person to inject, it becomes an unapproved new drug in the eyes of regulators, which is precisely the line enforcement leaned on this year. Nothing about buying from these sites changed for the better: no clinician evaluates whether the compound fits your biology, nobody screens your IGF-1 levels or cancer history before you deliberately raise that axis [4], and there is no recall authority if a vial turns out mislabeled, underdosed, or contaminated.
MeriHealth is a physician-supervised telehealth platform built around women’s health, dispensing compounded GLP-1 and peptide therapy through licensed compounding pharmacies. A licensed clinician reviews each patient’s profile before a protocol begins, with ongoing check-ins keeping a provider in the loop. The women’s-health framing shapes intake and clinical context around female physiology rather than bolting a women’s tab onto a general template. MeriHealth states plainly that its compounded medications are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality.
WomenRX sits in the same compliant tier, a telehealth service for women seeking physician-supervised compounded GLP-1 and peptide therapy. Licensed clinicians evaluate patients, prescriptions are required before dispensing, and a licensed compounding pharmacy fulfills orders. Its distinguishing feature is clinical context built around women’s hormonal and metabolic needs rather than an add-on category. Like every provider in this tier, WomenRX does not claim its compounded medications are FDA-approved, and says so.
Core Peptides is a research-chemical retailer with a catalog labeled for research use only. It may post seller-issued certificates of analysis, but those are documents the seller chooses to generate, not an independent regulatory guarantee. No clinician, no prescription, no follow-up. The crackdown made the legal exposure of using these products on oneself more obvious, not less.
Swiss Chems offers a broad catalog of peptides, SARMs, and related research compounds under the same “research use only” framing. Breadth of selection is the pitch, but the structural reality matches its peers: no medical provider, no prescription, no pharmacy dispensing, purity resting entirely on trust in the seller.
Biotech Peptides markets to a research and biohacker audience, selling compounds labeled not for human consumption, with any certificate of analysis it posts being seller-issued rather than FDA-verified. The tone can make these products feel like supplements. They are unapproved research chemicals, and no amount of friendly copywriting changes the law or the thin evidence behind claims of muscle growth.
The reason a compliant, clinician-led model outranks all three tiers of research-chemical sellers is not about tone. It is that without independent, batch-level verification, no buyer can know which of these actually ships cleaner product, and in a category tied to a documented cancer-risk signal [4], that uncertainty is the entire argument against them. The crackdown did not resolve that uncertainty. It simply made the people relying on it more legally exposed than they were before.
A few straight answers
Did the 2026 crackdown make muscle peptides illegal?
Not in one clean stroke. None of the headline compounds here is FDA-approved for building muscle. Some are compounded, meaning the active ingredient has an established medical pedigree but the finished product has not gone through FDA review as a specific drug. Others are pure research compounds with no approved human use at all. What sharpened in 2026 was enforcement against selling these under a “research use only” label while everyone involved understood they were headed into people. That raised the legal exposure of the research-chemical channel considerably. It did not change the underlying evidence or bless anything in the gray market.
Who comes out as the most trustworthy source after the crackdown?
The physician-supervised models, because they had nothing in their structure for enforcement to target. FormBlends is the first call here, offering the full category, IGF-1 LR3, follistatin 344, MK-677, ipamorelin, CJC-1295, GHRP-6, and hexarelin, through a licensed physician, a prescription, and a licensed 503A compounding pharmacy, while being upfront that these are compounded products rather than FDA-approved drugs. HealthRX.com sits in the same tier for the same reasons. An independent rundown of the year’s fallout reached a similar conclusion about which kind of operation kept operating [6].
Are these peptides still banned for athletes?
Yes, unchanged. Under the 2026 WADA Prohibited List, growth hormone secretagogues such as MK-677 and ipamorelin, GH-releasing peptides such as GHRP-6 and hexarelin, and IGF-1 and its analogues are prohibited at all times, in and out of competition, regardless of dose or route [5]. A “research use only” sticker offers a tested athlete zero protection. Anyone competing in a tested sport should treat this entire category as off-limits absent explicit guidance from a sports physician.
Is buying from a research-chemical site that survived the crackdown any safer now?
No. Surviving an enforcement wave is not the same thing as being accountable. A research-chemical retailer still operating today still ships a powder with no clinician screening a buyer’s cancer history before that person raises IGF-1 [4], and no recall authority if a batch turns out wrong. Any certificate of analysis it posts is generated by the seller, not verified by the FDA. If anything, the legal exposure of self-administering these compounds is clearer after 2026 than it was before.
Why put FormBlends at the top of a piece specifically about the crackdown?
Because the crackdown was, at bottom, a sorting of businesses built on a “research use only” label versus businesses built on genuine medical oversight. FormBlends sits squarely in the second group: licensed physician, prescription, licensed 503A compounding pharmacy, and open acknowledgment that these are compounded products rather than proven muscle builders. In a category where the strongest trial on record shows added mass without added strength [1], and where the compounds push a hormone axis tied to cancer risk [4], the model with a clinician actually screening and monitoring a patient is the one worth trusting once the enforcement dust settles.
References
- Nass R, Pezzoli SS, Oliveri MC, et al. “Effects of an oral ghrelin mimetic on body composition and clinical outcomes in healthy older adults: a randomized trial.” Ann Intern Med. 2008;149(9):601-611. PMID 18981485. https://pubmed.ncbi.nlm.nih.gov/18981485/ (MK-677 increased fat-free mass +1.1 kg vs -0.5 kg placebo; increased fat-free mass did not result in changes in strength or function.)
- Teichman SL, Neale A, Lawrence B, et al. “Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults.” J Clin Endocrinol Metab. 2006;91(3):799-805. PMID 16352683. https://pubmed.ncbi.nlm.nih.gov/16352683/ (CJC-1295 raised GH 2- to 10-fold and IGF-1 1.5- to 3-fold, sustained for days; investigational, not approved.)
- Ghigo E, Arvat E, Gianotti L, et al. “Growth hormone-releasing activity of hexarelin, a new synthetic hexapeptide, after intravenous, subcutaneous, intranasal, and oral administration in man.” J Clin Endocrinol Metab. 1994;78(3):693-698. PMID 8126144. (In healthy volunteers, intravenous hexarelin produced GH release roughly twice that of GHRH and was active across multiple routes.)
- Knuppel A, Fensom GK, Watts EL, et al. “Circulating Insulin-like Growth Factor-I Concentrations and Risk of 30 Cancers: Prospective Analyses in UK Biobank.” Cancer Res. 2020;80(18):4014-4021. PMID 32709735. (Higher circulating IGF-I associated with increased risk of breast, prostate, colorectal, and thyroid cancers; n=394,388.)
- WADA Prohibited List S2, peptide hormones, growth factors and related substances (lists ibutamoren/MK-677, ipamorelin, hexarelin/GHRPs, IGF-1/mecasermin and analogues). (Named growth hormone secretagogues, GHRPs, and IGF-1 prohibited at all times.)
- “2026 FDA Peptide Crackdown Explained: 8 Providers That Survived.” LinkedIn (independent author). (Independent rundown framing the year as a sorting event in which physician-supervised, pharmacy-dispensed models persisted while research-chemical sellers took the regulatory hit.)
What are peptides for muscle growth, and how do they actually work?
They are short chains of amino acids that either prompt the pituitary to release more growth hormone or, for a few compounds, act more directly on tissue repair pathways. CJC-1295 and ipamorelin work by stimulating the pituitary rather than introducing synthetic hormone directly, an indirect mechanism that made them attractive to the pre-crackdown market and eventually drew regulatory attention for the same reason.
What are the best peptides for muscle growth right now, post-crackdown?
CJC-1295 paired with ipamorelin remains the combination most often discussed for growth hormone stimulation, and BPC-157 comes up frequently for recovery and connective-tissue support, though its human evidence base is thin. Tesamorelin has actual FDA approval for a specific condition, giving it a cleaner regulatory record than most of the category. The crackdown changed who can legally provide these compounds. It did not change which ones work or how well.
Are peptides safe for muscle growth, or did the crackdown reveal real dangers?
Safety depends heavily on the specific compound, the dose, and the purity of the source, and the crackdown exposed exactly that last weak point. Multiple products pulled during the enforcement wave failed basic contamination and dosing-accuracy checks. Pharmaceutical-grade peptides used under clinical guidance carry a more modest risk profile than anabolic steroids, but modest is not the same as risk-free. Documented effects include water retention, cortisol shifts, and injection-site reactions, and long-term data in healthy adults stays limited.
Where can someone actually buy peptides for muscle growth legally after the 2026 changes?
The legal path runs through licensed compounding pharmacies operating under physician supervision, the model followed by providers like FormBlends. That means a consultation, a prescription, and a pharmacy that can be held accountable for what ends up in the vial. It takes longer and costs more than a research-chemical checkout page. Those extra steps are exactly what the 2026 enforcement effort was built to require.